The Journal of Clinical and Preventive Cardiology has moved to a new website. You are currently visiting the old
website of the journal. To access the latest content, please visit www.jcpconline.org.
Polyunsaturated Fatty Acids: Role in Prevention of Cardiovascular Disease and Enhancing their Efficacy in Indian Cooking
Volume 4, Apr 2015
S Y Mhaskar PhD, Purvi Varma RD MSc (Clinical Nutrition) Mumbai, India
J Clin Prev Cardiol 2015;4(2):42-9
Diet exerts a profound influence on blood lipids and lipoproteins and as such should always be a major component of strategies for the primary prevention of diseases in which lipids play an etiological role such as in coronary heart disease (CHD). The role of dietary fat in health has been under intensive research and debate during the past decades.
The effects of both the amount and quality of dietary fat have been studied intensively during the past decades. Previously, low-fat diets were recommended without much attention to the quality of fat, whereas there is general emphasis on the quality of fat in current guidelines. The quality of fat has been shown to have a significant effect on serum lipid profile and blood pressure as well as endothelial function and low-grade inflammation and has furthermore, been shown to affect the risk of CVD either in itself or as an important component of a health promoting diet (1).
The quality of fat is generally specified by the relative content of saturated fatty acids (SFA), monounsaturated (MUFA), and polyunsaturated fatty acids (PUFA) including the proportion or amount of essential fatty acids, i.e., linoleic acid (LA) and a-linolenic acid (ALA), as well as the proportion or amount of long-chain polyunsaturated (LCPUFA) n-3 fatty acids (n-3 LCPUFA), i.e., eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). These two essential fatty acids (EFAs) are the only sources for the production of important longer chain PUFAs such as prostaglandins; dynamic but short lived compounds that control blood vessels and other body functions. Arachidonic acid (AA) (20:4 n-6) a member of the n-6 PUFA, is another source of prostaglandins (PG). Eicosapentaenoic acid (EPA) (20:5 n-3), LN and docosahexaenoic acid (DHA) (C22) EFAs are called three PUFAs or n-3 omega PUFAs (n-3 series) (2). In addition, dietary ALA can be converted to the EPA and DHA. LA and ALA PUFAs are truly essential as our body cannot synthesize them therefore have to be obtained through the diet.
In human nutrition, the PUFA plays an important role due to their hypocholesterolemic action, reducing the risk of arteriosclerosis (3). Dietary fat affects blood serum cholesterol in humans and, consequently, can influence the occurrence of coronary heart disease.
Over 30 years ago, Keys and Hegsted made the landmark observation that variation in the concentration of serum cholesterol across seven different countries was positively related to the amount of energy derived from saturated fat. Conversely, they found that intake of PUFA was inversely related to serum cholesterol. From this, they were able to formulate equations that enabled them to predict the quantitative effect of saturated and polyunsaturated fat on serum cholesterol (4).
DC = (2.7 * DS)-(1.3 * DP) + 1.521/2
where DC = change in plasma cholesterol concentration:
DS = change in percentage of energy from saturated fat:
DP = change in percentage of energy from PUFA:
Z = dietary cholesterol (mg) per 1000 kcal
History
For at least 50 years, polyunsaturated fatty acids (PUFAs) have been studied intensively as nutrients that protect against cardiovascular disease (CVD).
In 1950s and 1960s, high linoleic acid vegetable oils were a mainstay of hypercholesterolemia treatment due to lack of cholesterol lowering drugs. The consumption of corn, sunflower, safflower, or soybean oils was started amongst such patients on a daily basis. The potential of linoleic acid to reduce CVD was put to a rigorous test in randomized clinical trials, and reduction in definite clinical cardiovascular endpoints was established in the range of 20–35%, in line with the serum cholesterol reduction that was achieved (5). Prospective epidemiological studies in very large populations confirmed that dietary linoleic acid is predictive of reduced CVD (6). Thus, one paradigm became established, that linoleic acid, an omega-6 PUFA, is cardio protective.
In 1956–1957, four research groups published convincing experiments showing that linoleic acid (18 carbons, 2 double bonds, omega-6) substantially reduced serum cholesterol, and it remains the most potent cholesterol-lowering nutrient (5).
Following the 1961 American Heart Association Central Committee Advisory Statement to replace saturated fat with PUFAs in the diet, food production companies began replacing the saturated fatty acids in processed foods with un-saturated fatty acid oils, especially soybean oil. As a result, vegetable oils, shortening and margarine were recommended as replacements for animal fats such as butter, cream and cheese. These changes led to a marked (two to three-fold) increase in dietary LA, an estimated 40% reduction in total n-3 LCPUFAs levels, and a large shift in the ratio of dietary n-6/n-3 C18 PUFAs consumed from ~5:1 to >10:1 (7).
Benefits of PUFAs
PUFAs have been claimed to have a broad range of beneficial effects including lowering cholesterol, decreasing the risk of arrhythmia, lowering the blood pressure, preventing diabetes in pregnancy, and beneficial effects on joints (relief of arthritis). Both omega-3 and omega-6 PUFA are precursors of hormone-like compounds, which are involved in many important biological and biochemical processes in human body. They are indispensable for the syntheses of prostaglandins, thromboxanes, prostacyclines and leukotrienes and take part in the transport and oxidation of choles-terol. PUFAs are important constituents of the phospholipids of all cell membranes. LA, ALA and their metabolic products, AA, EPA and DHA are crucial structural and functional components of cellular and intracellular membranes in the human body. Phospholipids play an essential role in membrane structure and function. PUFAs of both the n-6 and n-3 series are incorporated into membrane phospholipids. The length and degree of unsaturated FAs in membrane phospholipids are the main determinants of fluidity, transport systems, activity of membrane-bound enzymes, and susceptibility to lipid peroxidation. In this context, an altered fatty acid (FA) composition with reduced levels of PUFAs and increased contents of saturated FA (SFA), that consequently decrease the PUFA/SFA ratio in erythrocyte membranes, may be associated with lower membrane fluidity in patients with chronic diseases (Table 1) (8,9).
Metabolic Pathways of PUFAs
Omega-6 polyunsaturated fatty acids (PUFA) are precursors for a number of key mediators of inflammation. An inter-mediate arachidonic acid may undergo –
Cyclooxygenase pathway leading to the formation of prostaglandin and thromboxanes or
Lipoxygenase pathway to form leukotriene.
The 2 series of Prostaglandins (2-series PG) - PGD2, E2, F2, and I2 is a potent mediator of inflammation and cell prolifer-ation. T thromboxanes (especially, thromboxane A2) and leukotrienes are responsible for their immunosuppressive properties and for the generation of free oxygen radicals.
Dietary supplements rich in omega-3 PUFA reduce the concentrations of 2-series PG and increase the synthesis of 3-series PG (e.g., PGE(3)), which are believed to be less inflammatory. EPA, LN and DHA (n-3 omega PUFAs) helps to produce PGE1, a hormone in lipid origin which has got beneficial effects on the body, opposite to those of PGE2, such as regulation
Table 1. Potential beneficial effects of PUFA on physiological parameters
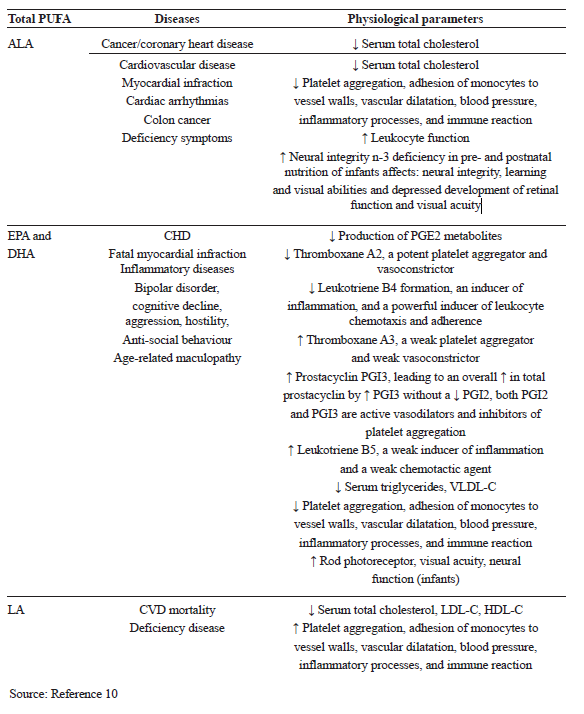
of calcium movement, controlling hormone regulation and cell growth, PGE3 and PGI3. PGE3 and PGI3 have got beneficial effects similar to those of PGE1, such as Source: Reference 10inhibiting inflammation and increasing 3 series PGs, thromboxane A3 and pentaenoic or 5 series leukotrienes (e.g. LTB5) (Figure 1) (11).

PUFA and Oxidation
It is known that the increase in the unsaturation in the fatty acids increases its vulnerability to oxidation during storage and cooking in geometric proportions and hence the n-6 and n-3 fatty acids undergo higher oxidation in presence of oxygen. Indian culinary practices involve deep frying which involves heating oil at 180°C and drying of the moisture at high temperature (12). At this temperature oil and its components comes in contact with the oxygen and water at very high temperature. These severe conditions lead to generation of free radicals which lead to breakdown of unsaturated fatty acids leading to harmful secondary oxidation products. Examples, also there is practice in India to recycle once used oils till 4-5 times and refill with fresh oil to maintain the optimal frying levels in pan which increase the content of secondary oxidation products. Thus the Indian deep frying practices are harmful to larger extent on nutritional quality of oils which is generally experienced by user as an off flavor, dark color and increased viscosity due to polymerization. The byproducts generated in due course of frying are many and a few of these malondialdehyde, ketones, 4-hydroxynonenal (HNE), hydro peroxides are known to be carcinogenic and detrimental to health (13). Hence it is im-portant to provide an antioxidant system in the oil in Indian scenario which can protect oil as much as possible against the oxidation.
Antioxidants
Oxidative stress is the key culprit in the pathogenesis of CVD. The ‘antioxidant hypothesis’ proposes that vitamin C, vitamin E, carotenoids and other antioxidant nutrients offer protection against CVD by decreasing oxidative damage (14).
Under oxidative stress conditions, exogenous antioxidant supplementation can be used for preventive and/or thera-peutic intervention of CVD (14). Fortification of oil with antioxidants can be helpful. Generally oil has some antioxidant added to prevent the oxidation, but since the mechanism of the oxidation are different at the shelf, while frying and in vivo so there is a need to create a system of specifically designed antioxidants based on re-dox combinations (15). A single antioxidant does not work efficiently to cover all the risks arising out.
Dietary Sources
LA is present in significant amounts in many vegetable oils, including corn, sunflower, safflower and soybean oils, and in products made from these oils, such as margarines. ALA is found in green plant tissues, in some common vegetable oils, including soybean and rapeseed oils, in nuts, green plants, botanical oils, such as flax seed oil. The richest sources of EPA, DPA and DHA are oily fish (tuna, salmon, mackerel, herring, and sardine).
In functional food development, incorporation of PUFAs into food products is dominated by omega-3 fatty acids (α-linolenic acid (ALA) C18:3n-3, eicosapentaenoic acid (EPA) C20:5n-3, docosahexaenoic acid (DHA) C22:6n-3) and omega-6 fatty acids (γ-linolenic acid (GLA) C18:3n-6 and arachidonic acid (AA) C20:4n-6). Soybean, canola, flaxseed, hemp are the major sources of ALA, while GLA is mostly found in evening primrose, blackcurrant and borage oils. Oils from the marine algae are mainly rich in DHA only, while fish oil contains both EPA and DHA.
Effect of PUFA on Cholesterol
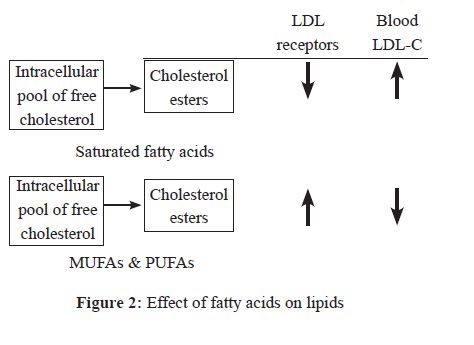
Consistent associations have been found between higher intakes of specific dietary fats, including particular polyunsaturated fatty acids, and between substituting (easily digested) carbohydrates with polyunsaturated fat, and lower risk of heart disease (16). A meta-analysis of 60 controlled trials reported that replacement of carbohydrates with PUFAs (largely n-6) had a beneficial effect on the total cholesterol/HDL-cholesterol ratio, and on the LDL concentration. Replacing SFA by n-6 PUFAs also led to a substantial reduction in the total cholesterol and LDL-cholesterol, a reduction of the total cholesterol/HDL-cholesterol ratio and thus may reduce the risk of CHD (Figure 2).
Monounsaturated fats are considered the healthiest type of fats. However, PUFA are better than saturated fatty ac-ids. They have shown to reduce LDL or bad cholesterol while increasing HDL or good cholesterol. A blend of MUFA and PUFA can help in bringing about a good fatty acid ratio and control the presence of excessive n-6 fatty acid. In this context various commercially available vegetable oils such as rice bran oil (RBO), safflower oil (SFO), soya bean oil (SBO) has been explored and studied extensively at our laboratory for its keeping quality and nutritional benefits in pre-clinical and clinical models. Out of several blends tested we have shown that refined Rice bran oil and Safflower oil blend in the ratio of (7:3 wt/wt) in keeping quality during frying and providing optimal nutritive value was effective and beneficial in preliminary studies which is concurrence with the previous study (19-23).
The edible oils formulated with antioxidant technology were tested for its keeping quality, shelf life using in vitro laboratory studies. Findings were very encouraging and the antioxidant technology was shown to provide triple benefit during frying, in increasing shelf life and helped for increased bioavailability by its virtue of PUFA content.
Thus in principle, a blend of RBO and SFO should be complementary with added antioxidant technology in keeping quality of oils and providing nutritional and health benefits. Also, a blend of these two oils (RBO and SO) should be complementary in lowering hyperlipidemia, and thereby control a known risk factor. This hypothesis has been tested in the present study.
Recommended Fatty Acid Intake
In line with authoritative international health bodies (WHO/FAO) and current evidence, the IEM supports the following recommendations for optimal lifelong health from age two years though adulthood (24):
Conclusion
There is convincing evidence that linoleic acid (LA) and alphalinolenic acid (ALA) are indispensable since they cannot be synthesized by humans. There is convincing evidence that replacing SFA with PUFA decreases the risk of CHD. There is convincing and sufficient evidence from experimental studies to set an acceptable intake to meet essential FA needs for LA and ALA consumption. There is possible evidence that PUFA affect the risk of alterations in indices related to the metabolic syndrome. There is possible evidence of a relationship between PUFA intake and reduced risk of diabetes (24).
References
The effects of both the amount and quality of dietary fat have been studied intensively during the past decades. Previously, low-fat diets were recommended without much attention to the quality of fat, whereas there is general emphasis on the quality of fat in current guidelines. The quality of fat has been shown to have a significant effect on serum lipid profile and blood pressure as well as endothelial function and low-grade inflammation and has furthermore, been shown to affect the risk of CVD either in itself or as an important component of a health promoting diet (1).
The quality of fat is generally specified by the relative content of saturated fatty acids (SFA), monounsaturated (MUFA), and polyunsaturated fatty acids (PUFA) including the proportion or amount of essential fatty acids, i.e., linoleic acid (LA) and a-linolenic acid (ALA), as well as the proportion or amount of long-chain polyunsaturated (LCPUFA) n-3 fatty acids (n-3 LCPUFA), i.e., eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA). These two essential fatty acids (EFAs) are the only sources for the production of important longer chain PUFAs such as prostaglandins; dynamic but short lived compounds that control blood vessels and other body functions. Arachidonic acid (AA) (20:4 n-6) a member of the n-6 PUFA, is another source of prostaglandins (PG). Eicosapentaenoic acid (EPA) (20:5 n-3), LN and docosahexaenoic acid (DHA) (C22) EFAs are called three PUFAs or n-3 omega PUFAs (n-3 series) (2). In addition, dietary ALA can be converted to the EPA and DHA. LA and ALA PUFAs are truly essential as our body cannot synthesize them therefore have to be obtained through the diet.
In human nutrition, the PUFA plays an important role due to their hypocholesterolemic action, reducing the risk of arteriosclerosis (3). Dietary fat affects blood serum cholesterol in humans and, consequently, can influence the occurrence of coronary heart disease.
Over 30 years ago, Keys and Hegsted made the landmark observation that variation in the concentration of serum cholesterol across seven different countries was positively related to the amount of energy derived from saturated fat. Conversely, they found that intake of PUFA was inversely related to serum cholesterol. From this, they were able to formulate equations that enabled them to predict the quantitative effect of saturated and polyunsaturated fat on serum cholesterol (4).
DC = (2.7 * DS)-(1.3 * DP) + 1.521/2
where DC = change in plasma cholesterol concentration:
DS = change in percentage of energy from saturated fat:
DP = change in percentage of energy from PUFA:
Z = dietary cholesterol (mg) per 1000 kcal
History
For at least 50 years, polyunsaturated fatty acids (PUFAs) have been studied intensively as nutrients that protect against cardiovascular disease (CVD).
In 1950s and 1960s, high linoleic acid vegetable oils were a mainstay of hypercholesterolemia treatment due to lack of cholesterol lowering drugs. The consumption of corn, sunflower, safflower, or soybean oils was started amongst such patients on a daily basis. The potential of linoleic acid to reduce CVD was put to a rigorous test in randomized clinical trials, and reduction in definite clinical cardiovascular endpoints was established in the range of 20–35%, in line with the serum cholesterol reduction that was achieved (5). Prospective epidemiological studies in very large populations confirmed that dietary linoleic acid is predictive of reduced CVD (6). Thus, one paradigm became established, that linoleic acid, an omega-6 PUFA, is cardio protective.
In 1956–1957, four research groups published convincing experiments showing that linoleic acid (18 carbons, 2 double bonds, omega-6) substantially reduced serum cholesterol, and it remains the most potent cholesterol-lowering nutrient (5).
Following the 1961 American Heart Association Central Committee Advisory Statement to replace saturated fat with PUFAs in the diet, food production companies began replacing the saturated fatty acids in processed foods with un-saturated fatty acid oils, especially soybean oil. As a result, vegetable oils, shortening and margarine were recommended as replacements for animal fats such as butter, cream and cheese. These changes led to a marked (two to three-fold) increase in dietary LA, an estimated 40% reduction in total n-3 LCPUFAs levels, and a large shift in the ratio of dietary n-6/n-3 C18 PUFAs consumed from ~5:1 to >10:1 (7).
Benefits of PUFAs
PUFAs have been claimed to have a broad range of beneficial effects including lowering cholesterol, decreasing the risk of arrhythmia, lowering the blood pressure, preventing diabetes in pregnancy, and beneficial effects on joints (relief of arthritis). Both omega-3 and omega-6 PUFA are precursors of hormone-like compounds, which are involved in many important biological and biochemical processes in human body. They are indispensable for the syntheses of prostaglandins, thromboxanes, prostacyclines and leukotrienes and take part in the transport and oxidation of choles-terol. PUFAs are important constituents of the phospholipids of all cell membranes. LA, ALA and their metabolic products, AA, EPA and DHA are crucial structural and functional components of cellular and intracellular membranes in the human body. Phospholipids play an essential role in membrane structure and function. PUFAs of both the n-6 and n-3 series are incorporated into membrane phospholipids. The length and degree of unsaturated FAs in membrane phospholipids are the main determinants of fluidity, transport systems, activity of membrane-bound enzymes, and susceptibility to lipid peroxidation. In this context, an altered fatty acid (FA) composition with reduced levels of PUFAs and increased contents of saturated FA (SFA), that consequently decrease the PUFA/SFA ratio in erythrocyte membranes, may be associated with lower membrane fluidity in patients with chronic diseases (Table 1) (8,9).
Metabolic Pathways of PUFAs
Omega-6 polyunsaturated fatty acids (PUFA) are precursors for a number of key mediators of inflammation. An inter-mediate arachidonic acid may undergo –
Cyclooxygenase pathway leading to the formation of prostaglandin and thromboxanes or
Lipoxygenase pathway to form leukotriene.
The 2 series of Prostaglandins (2-series PG) - PGD2, E2, F2, and I2 is a potent mediator of inflammation and cell prolifer-ation. T thromboxanes (especially, thromboxane A2) and leukotrienes are responsible for their immunosuppressive properties and for the generation of free oxygen radicals.
Dietary supplements rich in omega-3 PUFA reduce the concentrations of 2-series PG and increase the synthesis of 3-series PG (e.g., PGE(3)), which are believed to be less inflammatory. EPA, LN and DHA (n-3 omega PUFAs) helps to produce PGE1, a hormone in lipid origin which has got beneficial effects on the body, opposite to those of PGE2, such as regulation
Table 1. Potential beneficial effects of PUFA on physiological parameters
of calcium movement, controlling hormone regulation and cell growth, PGE3 and PGI3. PGE3 and PGI3 have got beneficial effects similar to those of PGE1, such as Source: Reference 10inhibiting inflammation and increasing 3 series PGs, thromboxane A3 and pentaenoic or 5 series leukotrienes (e.g. LTB5) (Figure 1) (11).
PUFA and Oxidation
It is known that the increase in the unsaturation in the fatty acids increases its vulnerability to oxidation during storage and cooking in geometric proportions and hence the n-6 and n-3 fatty acids undergo higher oxidation in presence of oxygen. Indian culinary practices involve deep frying which involves heating oil at 180°C and drying of the moisture at high temperature (12). At this temperature oil and its components comes in contact with the oxygen and water at very high temperature. These severe conditions lead to generation of free radicals which lead to breakdown of unsaturated fatty acids leading to harmful secondary oxidation products. Examples, also there is practice in India to recycle once used oils till 4-5 times and refill with fresh oil to maintain the optimal frying levels in pan which increase the content of secondary oxidation products. Thus the Indian deep frying practices are harmful to larger extent on nutritional quality of oils which is generally experienced by user as an off flavor, dark color and increased viscosity due to polymerization. The byproducts generated in due course of frying are many and a few of these malondialdehyde, ketones, 4-hydroxynonenal (HNE), hydro peroxides are known to be carcinogenic and detrimental to health (13). Hence it is im-portant to provide an antioxidant system in the oil in Indian scenario which can protect oil as much as possible against the oxidation.
Antioxidants
Oxidative stress is the key culprit in the pathogenesis of CVD. The ‘antioxidant hypothesis’ proposes that vitamin C, vitamin E, carotenoids and other antioxidant nutrients offer protection against CVD by decreasing oxidative damage (14).
Under oxidative stress conditions, exogenous antioxidant supplementation can be used for preventive and/or thera-peutic intervention of CVD (14). Fortification of oil with antioxidants can be helpful. Generally oil has some antioxidant added to prevent the oxidation, but since the mechanism of the oxidation are different at the shelf, while frying and in vivo so there is a need to create a system of specifically designed antioxidants based on re-dox combinations (15). A single antioxidant does not work efficiently to cover all the risks arising out.
Dietary Sources
LA is present in significant amounts in many vegetable oils, including corn, sunflower, safflower and soybean oils, and in products made from these oils, such as margarines. ALA is found in green plant tissues, in some common vegetable oils, including soybean and rapeseed oils, in nuts, green plants, botanical oils, such as flax seed oil. The richest sources of EPA, DPA and DHA are oily fish (tuna, salmon, mackerel, herring, and sardine).
In functional food development, incorporation of PUFAs into food products is dominated by omega-3 fatty acids (α-linolenic acid (ALA) C18:3n-3, eicosapentaenoic acid (EPA) C20:5n-3, docosahexaenoic acid (DHA) C22:6n-3) and omega-6 fatty acids (γ-linolenic acid (GLA) C18:3n-6 and arachidonic acid (AA) C20:4n-6). Soybean, canola, flaxseed, hemp are the major sources of ALA, while GLA is mostly found in evening primrose, blackcurrant and borage oils. Oils from the marine algae are mainly rich in DHA only, while fish oil contains both EPA and DHA.
Effect of PUFA on Cholesterol
Consistent associations have been found between higher intakes of specific dietary fats, including particular polyunsaturated fatty acids, and between substituting (easily digested) carbohydrates with polyunsaturated fat, and lower risk of heart disease (16). A meta-analysis of 60 controlled trials reported that replacement of carbohydrates with PUFAs (largely n-6) had a beneficial effect on the total cholesterol/HDL-cholesterol ratio, and on the LDL concentration. Replacing SFA by n-6 PUFAs also led to a substantial reduction in the total cholesterol and LDL-cholesterol, a reduction of the total cholesterol/HDL-cholesterol ratio and thus may reduce the risk of CHD (Figure 2).
Generally, when saturated fatty acids are replaced with PUFAs in the diet, total and LDL-cholesterol concentrations decrease. In some studies in which saturated fatty acids were replaced with n−6 PUFAs and the ratio of polyunsaturated to saturated fat increased, an HDL-cholesterol-lowering effect was shown, although not consistently. However, because LDL-cholesterol concentrations also decline with such n−6 PUFA–rich diets, the ratio of LDL to HDL cholesterol may not change significantly. When n−3 PUFAs were given as supplements to the habitual diet, LDL-cholesterol-raising effects were noted by some, whereas HDL-cholesterol
concentrations were unchanged or increased slightly. In the Shunt Occlusion Trial, daily supplementation of 4g highly purified n−3 PUFA concentrate/d did not significantly influence serum concentrations of total, HDL, or LDL cholesterol compared with the unsupplemented group. Such factors as characteristics of the subjects (i.e., their hyperlipidemic phenotypes and background diet) and of the study (i.e., the type of supplement given, time of follow-up, and design details) may affect study outcomes significantly (17).
Ratio of n-6 to n-3 PUFAs
The 'modern western' diet has increased the onset and progression of chronic human diseases as qualitatively and quantitatively maladaptive dietary components. There has been a three-fold increase in dietary levels of the omega-6 (n-6), polyunsaturated fatty acid (PUFA) linoleic acid, with the addition of cooking oils and processed foods (18).
The American Heart association (AHA) recommends the SFA:MUFA:PUFA ratio to be 1:1:1 for healthy individuals (19).
Studies have shown varying effects on plasma lipids by substituting dietary saturated fats with PUFA, MUFA and carbohydrates (Table 2).

Blend of PUFA Oilsconcentrations were unchanged or increased slightly. In the Shunt Occlusion Trial, daily supplementation of 4g highly purified n−3 PUFA concentrate/d did not significantly influence serum concentrations of total, HDL, or LDL cholesterol compared with the unsupplemented group. Such factors as characteristics of the subjects (i.e., their hyperlipidemic phenotypes and background diet) and of the study (i.e., the type of supplement given, time of follow-up, and design details) may affect study outcomes significantly (17).
Ratio of n-6 to n-3 PUFAs
The 'modern western' diet has increased the onset and progression of chronic human diseases as qualitatively and quantitatively maladaptive dietary components. There has been a three-fold increase in dietary levels of the omega-6 (n-6), polyunsaturated fatty acid (PUFA) linoleic acid, with the addition of cooking oils and processed foods (18).
The American Heart association (AHA) recommends the SFA:MUFA:PUFA ratio to be 1:1:1 for healthy individuals (19).
Studies have shown varying effects on plasma lipids by substituting dietary saturated fats with PUFA, MUFA and carbohydrates (Table 2).
Monounsaturated fats are considered the healthiest type of fats. However, PUFA are better than saturated fatty ac-ids. They have shown to reduce LDL or bad cholesterol while increasing HDL or good cholesterol. A blend of MUFA and PUFA can help in bringing about a good fatty acid ratio and control the presence of excessive n-6 fatty acid. In this context various commercially available vegetable oils such as rice bran oil (RBO), safflower oil (SFO), soya bean oil (SBO) has been explored and studied extensively at our laboratory for its keeping quality and nutritional benefits in pre-clinical and clinical models. Out of several blends tested we have shown that refined Rice bran oil and Safflower oil blend in the ratio of (7:3 wt/wt) in keeping quality during frying and providing optimal nutritive value was effective and beneficial in preliminary studies which is concurrence with the previous study (19-23).
The edible oils formulated with antioxidant technology were tested for its keeping quality, shelf life using in vitro laboratory studies. Findings were very encouraging and the antioxidant technology was shown to provide triple benefit during frying, in increasing shelf life and helped for increased bioavailability by its virtue of PUFA content.
Thus in principle, a blend of RBO and SFO should be complementary with added antioxidant technology in keeping quality of oils and providing nutritional and health benefits. Also, a blend of these two oils (RBO and SO) should be complementary in lowering hyperlipidemia, and thereby control a known risk factor. This hypothesis has been tested in the present study.
Recommended Fatty Acid Intake
In line with authoritative international health bodies (WHO/FAO) and current evidence, the IEM supports the following recommendations for optimal lifelong health from age two years though adulthood (24):
- Fat may provide from 20% up to 30-35% of the daily energy intake;
- Saturated fatty acids should provide no more than 10% of the daily energy intake;
- Essential polyunsaturated fatty acids (PUFA) (omega-6 and omega-3) should contribute 6-11 % of the daily energy intake;
- The omega-3 polyunsaturated alpha-linolenic acid (ALA) should provide 0.5%-2% of the daily energy intake.
- Adults should consume at least 250 mg/day of the long-chain omega-3 fatty acids eicosapentaenoic acid (EPA) and docosahexaenoic acid (DHA);
- The intake of trans fatty acids should be kept to a minimum and not exceed 1% of the daily energy intake;
- The remainder of the energy from fat can be provided by monounsaturated fatty acids.
Conclusion
There is convincing evidence that linoleic acid (LA) and alphalinolenic acid (ALA) are indispensable since they cannot be synthesized by humans. There is convincing evidence that replacing SFA with PUFA decreases the risk of CHD. There is convincing and sufficient evidence from experimental studies to set an acceptable intake to meet essential FA needs for LA and ALA consumption. There is possible evidence that PUFA affect the risk of alterations in indices related to the metabolic syndrome. There is possible evidence of a relationship between PUFA intake and reduced risk of diabetes (24).
References
- Schwab U, Lauritzen L, Tholstrup T, Haldorssoni T, Riserus U, Uusitupa M, Becker W. Effect of the amount and type of dietary fat on cardiometabolic risk factors and risk of developing type 2 diabetes, cardiovascular diseases, and cancer: a systematic review. Food Nutr Res. 2014 Jul 10;58. doi: 10.3402/fnr.v58.25145
- Pereira SL, Leonard AE, Mukerji P. Recent advances in the study of fatty acid desaturases from animals and lower eukaryotes. Prostaglandins Leukot Essent Fatty Acids. 2003;68:97-106.
- Ahrens Eh Jr, Insull W Jr, Blomstrand R, Hirsch J, Tsaltas TT, Peterson ML. The influence of dietary fats on serum-lipid levels in man. Lancet. 1957;272(6976):943-53.
- Keys A. Coronary Heart Disease in seven countries, American Heart Association Monograph No. 29, New York. American Heart Association. Circulation. 1970;41:1-21.
- Sacks FM, Katan M. Randomized clinical trials on the effects of dietary fat and carbohydrate on plasma lipoproteins and cardiovascular disease. Am J Med. 2002;113 Suppl 9B:13S-24S.
- Ascherio A. Epidemiologic studies on dietary fats and coronary heart disease. Am J Med. 2002;113 Suppl 9B:9S-12S.
- Wood DA, Riemersma RA, Butler S, Thomson M, Macintyre C, Elton RA, Oliver MF. Linoleic and eicosapentaenoic acids in adipose tissue and platelets and risk of coronary heart disease. Lancet. 1987;1(8526):177-83.
- Ferrucci L, Cherubini A, Bandinelli S, Bartali B, Corsi A, Lauretani F, Martin A, Andres-Lacueva C, Senin U, Guralnik JM.Relationship of plasma polyunsaturated fatty acids to circulating inflammatory markers. J Clin Endocrinol Metab. 2006;91:439-46.
- Bieniarz et al. Fatty acids, fat and cholesterol in some lines of Carp. Arch Pol Fish. 2001;9:5-24.
- Ristić-Medić D, Vučić V, Takić M, Karadić I, Glibetić M. Polyunsaturated fatty acid in health and disease. Journal of the Serbian Chemical Society 2013;78:1269–89.
- Gogus U, Smith C. n-3 Omega fatty acids: a review of current knowledgeInternational Journal of Food Science and Technology 2010;45:417–36.
- Ayala A, Muñoz MF, Argüelles S. Lipid peroxidation: production, metabolism, and signaling mechanisms of malondialdehyde and 4-hydroxy-2-nonenal. Oxid Med Cell Longev. 2014;2014:360438.
- Niki E. Assessment of antioxidant capacity in vitro and in vivo. Free Radic Biol Med. 2010;49:503-15.
- Wongama GP, Dirk JB, Adriaan JE, Guillaume A. Dietary antioxidant properties of vegetable oils and nuts – the race against cardiovascular disease progression. In: Antioxidant-Antidiabetic Agents and Human Health. ISBN 978-953-51-1215-0, Eds Oluwafemi Oguntibeju. Intech, Croatia. 2014;209-38.
- Mishra S, Manchanda SC. Cooking oils for heart health. Journal of Preventive Cardiology. 2012;1:123-31.
- Willett WC. The role of dietary n-6 fatty acids in the prevention of cardiovascular disease. J Cardiovasc Med (Hagerstown). 2007;8 Suppl 1:S42-5.
- Eritsland J. Safety considerations of polyunsaturated fatty acids. Am J Clin Nutr. 2000;71(1 Suppl):197S-201S.
- Chilton FH, Murphy RC, Wilson BA, Sergeant S, Ainsworth H, Seeds MC, Mathias RA. Diet-gene interactions and PUFA metabolism: a potential contributor to health disparities and human diseases. Nutrients. 2014;6:1993-2022.
- Hayes KC. Dietary fat and heart health: in search of the ideal fat. Asia Pac J Clin Nutr. 2002;11 Suppl 7:S394-400.
- Sugano M, Tsuji E. Rice bran oil and cholesterol metabolism. J Nutr. 1997;127:521S-524S
- Upadya H, Devaraju CJ, Joshi SR. Anti-inflammatory properties of blended edible oil with synergistic antioxidants. Indian J Endocrinol Metab. 2015;19:511-9.
- Malve H, Kerkar P, Mishra N, Loke S, Rege NN, Marwaha-Jaspal A, Jainani KJ. LDL-cholesterol lowering activity of a blend of rice bran oil and safflower oil (8:2) in patients with hyperlipidaemia: a proof of concept, double blind, controlled, randomised parallel group study. J Indian Med Assoc. 2010;108:785-8.
- National Institute of Nutrition: Use correct combination/blend of 2 or more vegetable oils. Reference: Nutrient Requirements and Recommended Dietary Allowances for Indians. Indian Council of Medical Research 2010:106.
- FAO report of an expert consultation on fats and fatty acids in human nutrition. Geneva, 2008.
- Joint FAO/WHO Expert Consultation on Fats and Fatty Acids in Human Nutrition, Interim Summary of Conclusions and Dietary Recommendations on Total Fat & Fatty Acids, November 10-14, 2008, WHO HQ, Geneva, accessed from http://www.fao.org/ag/agn/nutrition/docs/Fats%20and%20Fatty%20Acids%20Summar y.pdf
