The Journal of Clinical and Preventive Cardiology has moved to a new website. You are currently visiting the old
website of the journal. To access the latest content, please visit www.jcpconline.org.
Aortic Root Abscess - Diagnosis, Complications and Managment
Volume 3, Oct 2014
Veeraj V. Kalburgi DNB, Hyderabad, India
J Clin Prev Cardiol 2014;3(4):153-4
Introduction
Aortic root abscess is a complication of aortic valve infective endocarditis. Not uncommon, this is a devastating disease associated with high morbidity and mortality. It usually occurs in immune-compromised, debilitated patients with multiple co-morbidities or in I/V drug abusers either on native or on prosthetic valves. Early diagnosis and prompt surgical intervention goes a long way in treating such patients successfully. Echocardiography plays a key role in early detection of this dreaded complication. We report here a patient of native valve endocarditis of aortic valve complicated with formation of aortic root abscess.
Case Summary
Aortic root abscess is a complication of aortic valve infective endocarditis. Not uncommon, this is a devastating disease associated with high morbidity and mortality. It usually occurs in immune-compromised, debilitated patients with multiple co-morbidities or in I/V drug abusers either on native or on prosthetic valves. Early diagnosis and prompt surgical intervention goes a long way in treating such patients successfully. Echocardiography plays a key role in early detection of this dreaded complication. We report here a patient of native valve endocarditis of aortic valve complicated with formation of aortic root abscess.
Case Summary
A 45 years old male, an agricultural laborer by occupation, presented with history of fever for the past 2 months along with shortness of breath for the past 15 days. Fever was associated with chills and rigors which did not improve despite local treatments. His breathlessness, which was on routine activities initially, had progressed during the past few days accompanied with episodes of PND for 5 days before presentation.
There were no similar complaints in the past. He was not a known hypertensive or diabetic. There was no history of intravenous drug abuse but he had been a chronic smoker and alcoholic for the past 15 years.
On examination, the patient looked pale and emaciated, with a BMI of 17.3kg/m2. Grade 2 clubbing was present but there was no icterus, cyanosis, pedal edema or lymphadenopathy. There were no stigmata of Infective endocarditis. His temperature was 102 degrees Fahrenheit, with pulse rate of 100/min and BP 90/40mmHg.Cardiac examination revealed normal JVP with cardiomegaly. LV S3 was audible along with a soft blowing early diastolic murmur in neoaortic area and a systolic flow murmur in the aortic area.
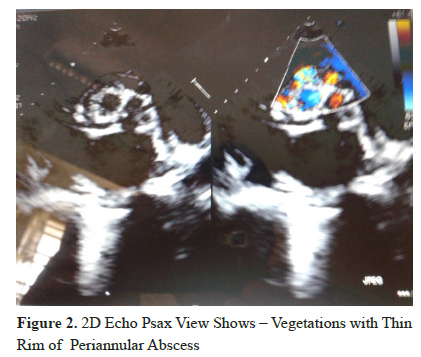
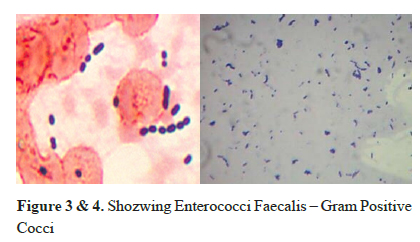
His investigations revealed severe anemia and leucocytosis (Hb - 7.1gm/dl, TLC – 15000/ml, Neutrophils predominating). Urine examination showed abundant red blood cells. His RFT and LFT were normal. ECG showed LVH with volume overload pattern. Chest X ray showed cardiomegaly. 2D echo showed vegetation on the aortic valve with an aortic root abscess causing severe AR with mild MR but with good LV function (Figures 1 & 2). Blood cultures showed growth of enterococcus faecium (Figures 3 & 4) which was sensitive to Vancomycin and Linezolid (but resistant to Pencillin, Aminoglycosides and Fluoroquinolones).
His investigations revealed severe anemia and leucocytosis (Hb - 7.1gm/dl, TLC – 15000/ml, Neutrophils predominating). Urine examination showed abundant red blood cells. His RFT and LFT were normal. ECG showed LVH with volume overload pattern. Chest X ray showed cardiomegaly. 2D echo showed vegetation on the aortic valve with an aortic root abscess causing severe AR with mild MR but with good LV function (Figures 1 & 2). Blood cultures showed growth of enterococcus faecium (Figures 3 & 4) which was sensitive to Vancomycin and Linezolid (but resistant to Pencillin, Aminoglycosides and Fluoroquinolones).
Discussion
Aortic root abscess in patients with aortic endocarditis is not uncommon. Aortic root abscess may cause persistent sepsis, heart failure, conduction abnormalities, fistula formation, and an increased need for surgery (1).
Perivalular Abscesses occur in 10-15% of NVE & 60% of PVE in Aortic valve Infection.
It should be suspected in any patient with aortic valve endocarditis who fails to improve within 72 hours on appropriate antibiotics, particularly with prosthetic valve infection. Persistence or recrudescence of fever, persistently raised white blood cell counts, and other markers of systemic inflammation or the development of cutaneous manifestations or embolic phenomena
Furthermore, trans-esophageal echocardiography (TEE) provides useful anatomical definitions like the extent of annular involvement, extension of abscess to involve the sub-aortic curtain or upper inter-ventricular septum. All these are very important considerations for planning surgery in these patients (3). Once an aortic root abscess is detected, urgent surgery is required. Aggressive debridement of all infected and devitalized tissue is the mainstay of the surgical treatment of aortic root abscess. Reconstruction of the left ventricular outflow tract with antilogous pericardium or translocation of the aortic valve may also be required. The use of biological material has clear advantages in this scenario. Aortic valve homo-grafts are particularly useful for several reasons: they enable the abscess cavity to be completely excluded from the circulation; they avoid the use of prosthetic material; and they are more resistant to infection than any other valve substitute (4).
References
It should be suspected in any patient with aortic valve endocarditis who fails to improve within 72 hours on appropriate antibiotics, particularly with prosthetic valve infection. Persistence or recrudescence of fever, persistently raised white blood cell counts, and other markers of systemic inflammation or the development of cutaneous manifestations or embolic phenomena
Furthermore, trans-esophageal echocardiography (TEE) provides useful anatomical definitions like the extent of annular involvement, extension of abscess to involve the sub-aortic curtain or upper inter-ventricular septum. All these are very important considerations for planning surgery in these patients (3). Once an aortic root abscess is detected, urgent surgery is required. Aggressive debridement of all infected and devitalized tissue is the mainstay of the surgical treatment of aortic root abscess. Reconstruction of the left ventricular outflow tract with antilogous pericardium or translocation of the aortic valve may also be required. The use of biological material has clear advantages in this scenario. Aortic valve homo-grafts are particularly useful for several reasons: they enable the abscess cavity to be completely excluded from the circulation; they avoid the use of prosthetic material; and they are more resistant to infection than any other valve substitute (4).
References
- Prashanth Panduranga Hindawi Publishing Corporation Case Reports in Critical Care Volume 2013, Article ID 636519, 3 pages http://dx.doi. org/10.1155/2013/636519
- Wong CM, Oldershaw P, Gibson DG(1981) Echocardiographic demonstration of aortic root abscess after infective endocarditis. Br Heart J 46:584–586.
- S J D BRECKER, J R PEPPER and S J EYKYN, AORTIC ROOT ABSCESS HEART 1999 82 : 260-262.
- Wong CM, Oldershaw P, Gibson DG. Echocardiographic demonstration of aortic root abscess after infective endocarditis. Br Heart J 1981;46:584–6.
