The Journal of Clinical and Preventive Cardiology has moved to a new website. You are currently visiting the old
website of the journal. To access the latest content, please visit www.jcpconline.org.
Idiopathic Right Atrial Enlargement with Sinus Node Dysfunction
Volume 4, Jan 2015
S. R. Mittal, DM Cardiology, Ajmer, India
J Clin Prev Cardiol. 2015;4(1):21-3
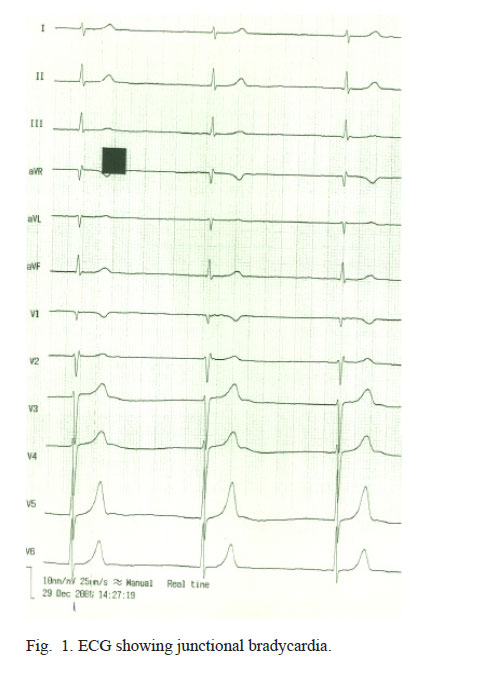
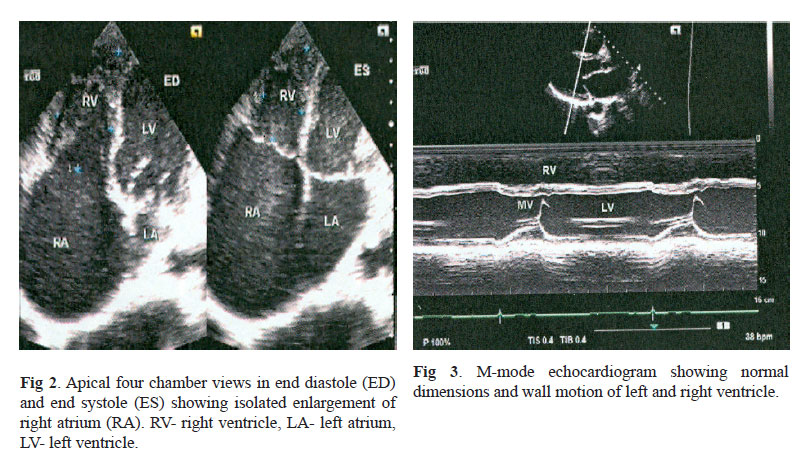
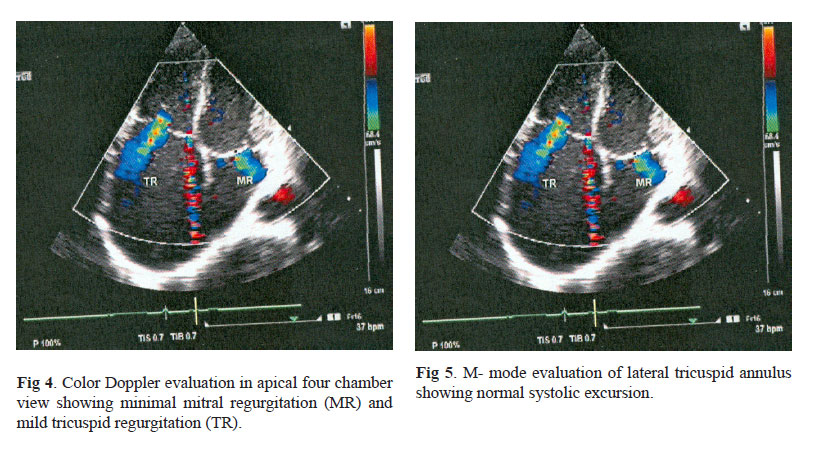
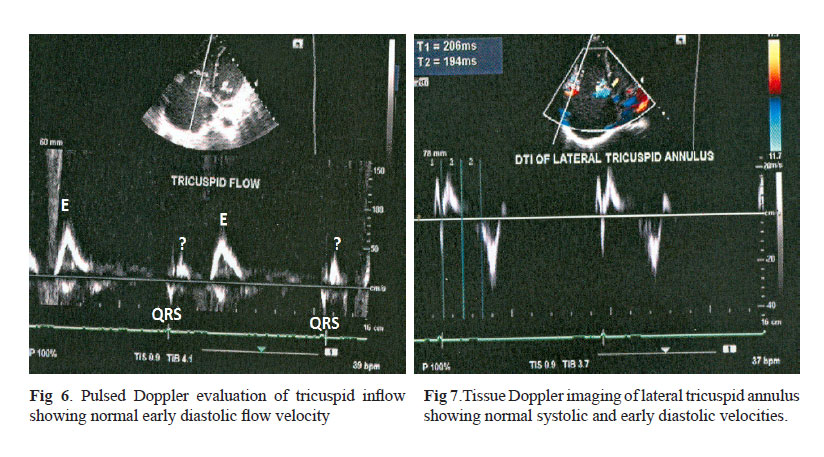
A 43-year-old asymptomatic male was referred for cardiac evaluation for bradycardia. Pulse rate was 34/ minute. Rest of the clinical examination was normal. Electrocardiogram revealed regular slow junctional rhythm at a rate of around 34/ minute. P wave was not visible and QRS was narrow (0.08 sec) (Fig 1). On Holter monitoring there was no atrial activity and QRS rate varied between 34 to 38/ minute. Patient did not agree for further evaluation. However, there was no change in pulse rate after walking for six minutes. Echocardiography revealed unexplained isolated enlargement of right atrium (Fig 2). Other cardiac chambers were normal (Fig 3). All cardiac valves were normal. There was no evidence of pulmonary artery hypertension. Color Doppler evaluation revealed mild tricuspid regurgitation and minimal mitral regurgitation (Fig 4). Tricuspid annulus plane systolic excursion was 31 .3 mm (Fig 5). Doppler evaluation of tricuspid flow revealed normal early diastolic filling E wave (Fig 6). There was no A wave before QRS. A small forward flow wave (marked?) was seen during early systole (after QRS of simultaneously recorded ECG). This could be because of continuing forward flow against closing tricuspid valve. Possibility of retrograde, atrial activation cannot be ruled out although no inverted P wave was visible during systole. Doppler tissue imaging of lateral tricuspid annulus revealed normal systolic and early diastolic velocities (Fig 7). There was no A’ wave. Pulsed Doppler evaluation of mitral inflow and tissue Doppler imagining of lateral and medial mitral annulus also did not reveal any atrial activity. Patient could not afford electrophysiological study. Possibility of unexcitable right atrium could not be ruled out. Patient did not agree for permanent pacemaker. Isolated enlargement of right atrium and accompanying sinus node dysfunction/ unexcitability of right atrium could be congenital.