The Journal of Clinical and Preventive Cardiology has moved to a new website. You are currently visiting the old
website of the journal. To access the latest content, please visit www.jcpconline.org.
Effectiveness of Planned Teaching Program on Angina Pectoris Among the Middle-aged People (35-60 Years)
Volume 2, Apr 2013
Juniya Bridgit Tomy MSc (Nursing)
J Clin Prev Cardiol. 2013;2(2):60-3
Introduction
Coronary artery disease (CAD) is the most prevalent type of cardiovascular disease (1). Coronary artery disease refers to the development and progression of plaque in the coronary arteries. Patients with coronary artery disease (CAD) often seek healthcare after experiencing angina or myocardial infarction (2). Second half of the 20th century has witnessed a global spread of the coronary artery disease (CAD) epidemic, especially in developing countries, including India. The high rates of coronary artery disease (CAD) in urban India compared to rural, despite lower rates of smoking, suggest important roles for nutritional and environmental factors. There is a significant increase in body mass index (BMI) in urban India compared to rural (BMI 24 kg/m2 versus 20 kg/m2 in men, 25 kg/m2 versus 20 kg/m2 in women) (3). WHO estimates 17 million people worldwide die of comcardiovascular disease each year and 60% of total cardiac patients is in India by 2010 (4).
Objectives
- To determine the pretest knowledge regarding angina pectoris among middle-aged people of a rural area.
- To evaluate the effectiveness of planned teaching program on angina pectoris in terms of gain in knowledge by posttest scores.
- To find out the association between pretest knowledge scores and selected demographic variables.
Hypotheses
All hypotheses were tested at 0.05 level of significance.H1: The mean posttest knowledge score of middle -aged rural people regarding angina pectoris will be significantly higher than their mean pretest knowledge score.
H2: There will be significant association between mean pretest knowledge scores of middle-aged rural people and selected demographic variables such as age, gender, educational status and socio-economic status.
Methodology
An evaluative approach with one group pretest, posttest, pre experimental design was used for the study. The sample consisted of 50 middle-aged rural people of selected rural area and was selected using convenience sampling technique. The data was collected usinga demographic proforma and structured knowledge questionnaire. The planned teaching program was administered after the pretest and the posttest were conducted on the seventh day using the same tool.
Data collection procedure
The permission for conducting the study was obtained from the Medical Officer, Primary Health Centre, Kateel, Mangalore. Consent to participate in the study was obtained from each subject. The ethical clearance for conducting the study was obtained from the ethicalcommittee of the institution. Subjects were selected according to the selection criteria of the study. On the first day to assess the knowledge of middle-aged rural people a pretest with structured knowledge questionnaire was conducted and after collecting the data, the planned teaching program (PTP) was administered on the same day. On the seventh day, a posttest with the same structured knowledge questionnaire was conducted to evaluate the effectiveness of the planned teaching program (PTP).
Data analysis
Data was analyzed using both descriptive and inferential statistics. Distribution of subjects with respect to the variables was represented using frequencies and percentage. Mean, standard deviation and mean percentage was used to describe knowledge of the middle-aged rural people, one group pretest (x) and posttest (y) preexperimental design was used to evaluate the effectiveness (y – x) of planned teaching program (PTP). Further statistical significance of the effectiveness of the planned teaching program (PTP) was analyzed by paired ‘t’ test.
Analysis and interpretation of data gathered was done based on the objectives and hypotheses of the study, using descriptive and inferential statistics.
Analysis and interpretation of data gathered was done based on the objectives and hypotheses of the study, using descriptive and inferential statistics.
Results
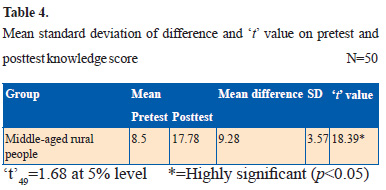
The mean posttest knowledge score (17.78) was higher than the mean pretest knowledge score (8.5). The posttest score ranged from 12 to 24 and the pretest score ranged from 4-13, respectively. The mean difference between posttest and pretest knowledge score was significant (t49=18.39) (t49=1.68 at 0.05 level). There was no association between pretest knowledge score and selected variables like age, gender, educational status, and socio-economic status.
Knowledge assessment indicates that 13 (26%) subjects’ knowledge score ranged from 7-8 in the pre-test, whereas 13 (26%) subjects’ knowledge score ranged from 17-18 in the posttest and it is analyzed using descriptive statistics as presented in Table 1.
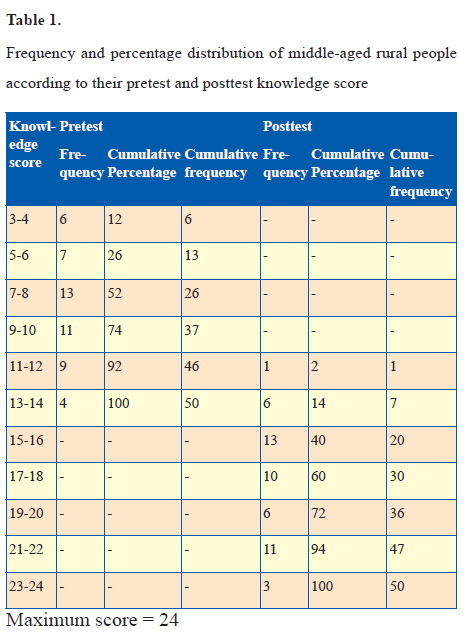
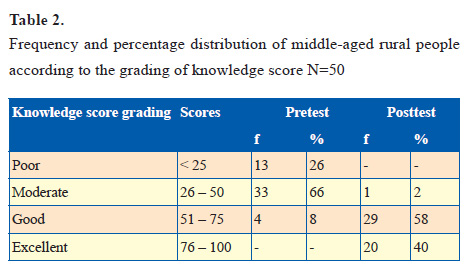
The range of post-test knowledge score (12-24) was higher than that of the pretest knowledge score (4-13) and the mean posttest knowledge score (17.78) was higher than the mean pretest knowledge score (8.50). Further the score of pretest and posttest were arbitrarily graded and the data is presented in Table 2. Highest percentage (66%) of the sample attained moderate level of knowledge score in the pretest, whereas in the posttest 58% of the sample had gained good knowledge score.
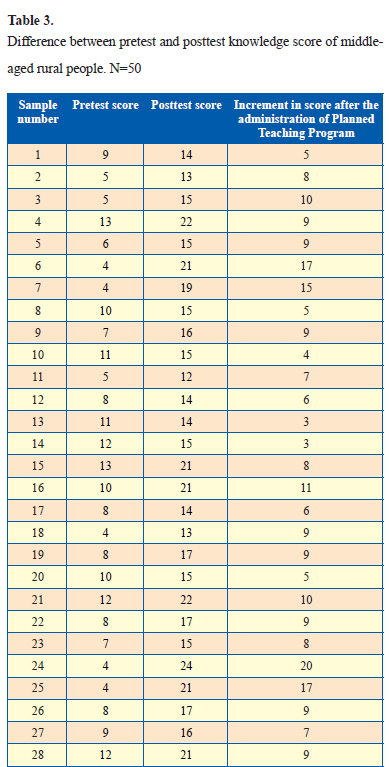
The difference between pretest and posttest knowledge score of each individual along with increment in knowledge score is presented in Table 3.

References
Knowledge assessment indicates that 13 (26%) subjects’ knowledge score ranged from 7-8 in the pre-test, whereas 13 (26%) subjects’ knowledge score ranged from 17-18 in the posttest and it is analyzed using descriptive statistics as presented in Table 1.
The range of post-test knowledge score (12-24) was higher than that of the pretest knowledge score (4-13) and the mean posttest knowledge score (17.78) was higher than the mean pretest knowledge score (8.50). Further the score of pretest and posttest were arbitrarily graded and the data is presented in Table 2. Highest percentage (66%) of the sample attained moderate level of knowledge score in the pretest, whereas in the posttest 58% of the sample had gained good knowledge score.
The difference between pretest and posttest knowledge score of each individual along with increment in knowledge score is presented in Table 3.
In order to find out the significant difference between pretest and posttest knowledge score paired ‘t’ was computed and data is presented in Table 4. The mean post-test knowledge score (17.78) was higher than the mean pre-test knowledge score (8.5). The computed ‘t’ value (t49 =18.39) was higher than the table value at 5% level. Hence, the null hypothesis H01 was rejected and the research hypothesis was accepted.
To test the statistical significance the following null hypothesis was stated:
H01: The mean posttest knowledge scores of middle-aged rural people will not be significantly higher than the mean pre-test knowledge score at 0.05 level.
χ-square (χ2) test was computed to test the association and the result is presented in Table 5.

χ-square (χ2) test was computed to test the association and the result is presented in Table 5.
The χ2 test showed that there was no significant association between pretest knowledge score of middle aged rural people compared with age, gender, educational status and socio-economic status (p<0.05) and it can be interpreted that the difference in mean score values related to the demographic variables were only by chance and not true.
Discussion
The role of nursing professional is crucial in giving health education and creating awareness among the community. By creating awareness among the public the nurse can break the chain of embarrassment and develop consciousness to give importance to their health.
Forty four percent of middle aged rural people were in the age group of 55 years and above and most of them 72% were females. Fifty eight percent of them were Hindus and an equal percentage had only primary education. Forty two percent of subjects belonged to the middle income group. Sixty four percent of the subjects were ignorant about angina pectoris.
The mean post-test knowledge score (17.78) was higher than the mean pretest knowledge score (8.50). The score ranged from 12-24 in the posttest and 4-13 in the pretest.
Findings of the present study showed that there was no significant association between knowledge and selected variables such as age, gender, educational status and socio-economic status, i.e.; age (χ2=0.403), gender (χ2=0.123), educational status (χ2=0.052), socio-economic status (x2 =1.173) at 0.05 level of significance.
Therefore, it is concluded that baseline factors are independent of their pretest level of knowledge on angina pectoris.
In the present study, knowledge of middle aged rural people on angina pectoris was not up to the mark before the administration of planned teaching program. The administration of planned teaching program on angina pectoris facilitated the middle-aged rural people to improve their knowledge on angina pectoris, which was evident in the posttest knowledge score.
Interpretation and Conclusion
Findings of the study have shown that the knowledge score of middle aged rural people was low before the administration of planned teaching program. The planned teaching program facilitated them to gain more knowledge regarding angina pectoris which was evident in post-test knowledge score. Hence, it can be concluded that the planned teaching program is an effective teaching strategy in improving the knowledge of middle-aged rural people regarding angina pectoris.
References
- Connell SC. Brunner and Suddarth’s Textbook of Medical-Surgical Nursing. 10th ed. Philadelphia: Lippincott Williams & Wilkins; 2003.
- Monahan F, Sands J, Marek J, Neighbours M. Medical-surgical nursing: Health and illness perspectives. 7th ed. United States: Elsevier Science Health Science; 2003.
- Singh SP, Sen P. Coronary Heart Disease: changing scenario. Indian J Prev Soc Med. 2003;34:1-2.
- Black JM, Hawks JH. Medical surgical nursing: Clinical management for positive outcomes. 7th ed. India: Thomson Press (India) Ltd; 2005.
